What Is VHL Disease?
Tumor growth may start affecting people with VHL disease in young adulthood and can persist throughout their lives1–3


Chronic and unpredictable tumor growth may affect multiple organ systems simultaneously3,5
When tumors are discovered by an HCP who specializes in 1 organ system, tumors may be developing elsewhere in the body3,5

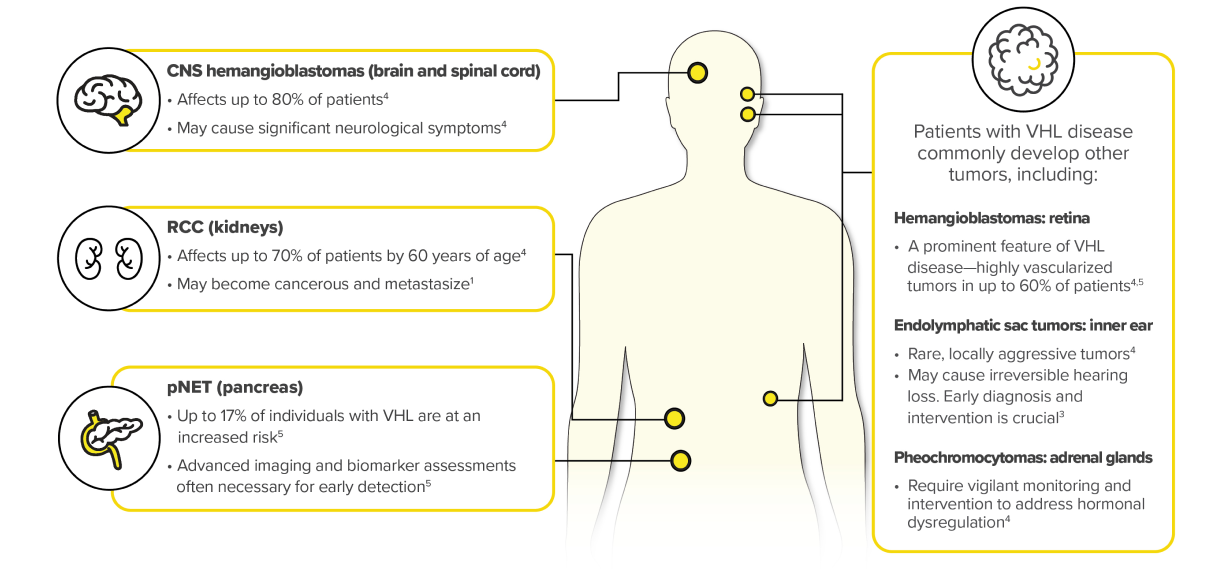
The systemic, recurrent, and unpredictable nature of VHL disease–associated tumors warrants vigilant surveillance and different management approaches3
VHL = von Hippel-Lindau; RCC = renal cell carcinoma; CNS = central nervous system; pNET = pancreatic neuroendocrine tumors; HCP = health care professional.
References: 1. National Organization for Rare Disorders. Von Hippel-Lindau disease. https://rarediseases.org/rare-diseases/von-hippel-lindau-disease/. Accessed November 13, 2023. 2. Maher ER, Yates JR, Harries R, et al. Clinical features and natural history of von Hippel-Lindau disease. Q J Med. 1990;77(283):1151–1163. 3. Binderup MLM, Smerdel M, Borgwadt L, et al. von Hippel-Lindau disease: Updated guideline for diagnosis and surveillance. Eur J Med Genet. 2022;65(8):104538. 4. Varshney N, Kebede AA, Owusu-Dapaah H, et al. A review of von Hippel-Lindau syndrome. J Kidney Cancer VHL. 2017;4(3):20–29. 5. Ganeshan D, Menias CO, Pickhardt PJ, et al. Tumors in von Hippel–Lindau syndrome: from head to toe—comprehensive state-of-the-art review. RadioGraphics. 2018;38(3):849–866. 6. What you need to know about VHL: a reference handbook for people with von Hippel-Lindau, their families, and their medical teams. 6th Ed. VHL Alliance. Revised 2020. https://www.vhl.org/wp-content/uploads/2022/12/vhla-handbook-2020.pdf. Accessed April 21, 2024. 7. Wolters WPG, Dreijerink KMA, Giles RH, et al. Multidisciplinary integrated care pathway for von Hippel-Lindau disease. Cancer. 2022;128(15):2871–2879.
Learn more about WELIREG: